

How to Automate Clinical Trial Operations Using Multi-Agent AI Systems
$150.00
| System Name: |
Autonomous Clinical Operations Management |
|---|---|
| Architecture: |
Hierarchical Multi-Agent System – 1 Trial Orchestrator (Coordinator) + 7 specialized Worker Agents (Protocol; Site Selection; Enrollment; Data Management; Safety; Regulatory; Budget) operating through clinical trial lifecycle stage management; shared clinical trial vector knowledge base; and human-in-the-loop approval gates at every regulatory; safety; and protocol decision point; 8 total agents |
| Coordinator Agent: |
Trial Orchestrator – maintains the master trial timeline and milestone risk register across all 7 Worker Agents; decomposes each trial phase (design; site activation; enrollment; data collection; closeout; submission) into domain-specific sub-tasks per Worker Agent; enforces trial lifecycle dependencies (Regulatory Agent must confirm IND clearance before Site Selection Agent activates sites; Safety Agent must process all outstanding adverse events before Regulatory Agent initiates NDA submission); monitors each agent’s milestone progress against the trial timeline; flags critical path delays to the VP Clinical Operations; and routes safety; protocol; and regulatory decisions to the appropriate Principal Investigator or CMO for mandatory human review |
| Worker Agents: |
Data Management Agent: Monitors EDC data quality and protocol adherence continuously – detecting missing data points, out-of-range values, and query trends in Medidata Rave EDC, classifying data issues by severity and impact on trial integrity, and generating data management queries for site resolution within configured SLA windows; Safety Agent: Processes adverse event (AE) and serious adverse event (SAE) reports – classifying each event by causality and severity using ICH E2A/E2B classification standards from the Knowledge Base, computing regulatory notification timelines (15-day for unexpected SAEs, 7-day for fatal/life-threatening), and routing all safety narratives to the Medical Monitor and Safety Committee for mandatory human review before any regulatory notification is submitted, Protocol Agent: Manages protocol development, version control, and amendment lifecycle – tracking protocol deviation incidents in the CTMS, identifying recurring deviation patterns that require protocol amendments, drafting amendment language using the Knowledge Base approved language library, and routing amendments to the Medical Monitor and IRB/Ethics Committee for mandatory review before any protocol change is implemented, Regulatory Agent: Prepares regulatory submission packages for IND applications, protocol amendments, NDA/BLA/MAA modules, and progress reports – assembling the required documents from Veeva CTMS, Medidata EDC, LIMS, and the Document Intelligence Knowledge Base, mapping each document to the applicable eCTD module, and routing the assembled package to the Regulatory Affairs Director for final review before submission; Budget Agent: Tracks trial costs vs. approved budget – monitoring site payment milestones, CRO invoices, investigator fees, and pass-through costs against the approved trial budget in the financial DW, computing cost-per-patient and cost-per-milestone metrics, identifying budget variance trends, and alerting the Clinical Program Director when projected trial cost exceeds the approved budget by more than the configured variance threshold, Site Selection Agent: Identifies and ranks optimal clinical trial sites for the target patient population – analyzing site performance data from prior trials (enrollment velocity, protocol deviation rate, data quality score, investigator experience with the indication), scoring site candidates against the trial’s enrollment criteria and geographic requirements, and presenting a ranked site shortlist to the Clinical Program Director for human selection; Enrollment Agent: Sources and engages eligible patients across configured channels – matching EHR patient records via FHIR API against inclusion/exclusion criteria, managing patient outreach communications through approved contact channels, tracking enrollment funnel metrics per site, and alerting the Enrollment Manager when site-level enrollment is falling behind the trial milestone plan |
| Extensibility Note: |
Beyond the 9 native Goldfinch AI tools; users can add custom tools self-service – including eTMF (electronic Trial Master File) platform connectors (Veeva Vault eTMF; OpenText); randomization and trial supply management (RTSM/IWRS) system connectors; patient-reported outcome (PRO) platform connectors (Medidata Patient Cloud); biomarker data management connectors; and real-world evidence (RWE) database APIs for synthetic control arm development. |
| On-Premise Supported: |
Yes – eZintegrations connects to on-premises systems (on-premises Veeva CTMS; on-premises Medidata EDC; on-premises LIMS; on-premises eTMF systems) via IPSec Tunnel. eZintegrations is a browser-based; cloud-hosted platform and does not require any on-premises software installation. |
| Tags: |
Goldfinch AI clinical operations; clinical trial AI orchestration; CTMS AI automation; adverse event AI agent; clinical trial enrollment AI; regulatory submission AI; EDC data quality AI; site selection AI agent; NDA submission AI; Veeva CTMS AI; Medidata AI integration; Goldfinch AI pharma |
| AI Credits Required: |
Yes – Document Intelligence is the primary credit consumer per trial due to the document-intensive nature of clinical trial operations (protocols, SAE narratives, regulatory guidance documents, prior submission packages). Credit consumption scales with trial complexity, phase, and document volume. |
| Safety Layer: |
Enrollment Agent’s inclusion/exclusion matching confidence falls below 0.80 for any patient candidate – Clinical Research Associate review required before patient outreach; Trial Orchestrator cross-agent confidence falls below 0.75 on any milestone risk assessment. Max 3 retries before VP Clinical Operations escalation. All HITL decisions logged with reviewer identity, decision, patient/site/submission reference, and timestamp for FDA 21 CFR Part 11, ICH E6 GCP, and ICH E2A audit documentation., Human-in-the-loop gate triggers when: Safety Agent classifies any adverse event as an SAE – Medical Monitor and Safety Committee review required before any regulatory notification is submitted; causality and expectedness assessment requires qualified physician review at all times; Protocol Agent identifies a protocol deviation requiring a protocol amendment – Medical Monitor and IRB/Ethics Committee approval required before any amendment is implemented; Regulatory Agent completes a submission package – Regulatory Affairs Director and CMO review and sign-off required before any submission to FDA, EMA, or other regulatory authority; |
| Goldfinch AI Native Tools Used: |
API Tool Call: All 7 Worker Agents use API Tool Call – Protocol Agent (Veeva CTMS https://www.veeva.com/products/vault-ctms/ protocol version and deviation tracking, IRB/Ethics Committee submission portal), Enrollment Agent (FHIR API https://www.hl7.org/fhir/ for EHR patient matching at configured sites, Veeva CTMS enrollment tracking), Data Management Agent (Medidata Rave EDC https://www.medidata.com/products/clinical-data-management/ data query API, LIMS https://www.labware.com/ sample data validation), Safety Agent (Veeva CTMS SAE module API, FDA MedWatch https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program and EMA EudraVigilance https://www.ema.europa.eu/en/human-regulatory-overview/research-and-development/pharmacovigilance/eudravigilance notification portal APIs), Regulatory Agent (FDA ESG electronic submissions gateway, Data Analysis: Enrollment Agent computes enrollment velocity per site and projects enrollment completion date vs. milestone; Site Selection Agent scores site candidates against weighted selection criteria; Data Management Agent classifies EDC data issues by severity and query response rate; Safety Agent computes SAE regulatory notification deadline from event date; Budget Agent computes cost variance, cost-per-patient, and projected trial cost overrun; Trial Orchestrator computes critical path milestone delay risk and trial completion date probability, Data Analytics with Charts/Graphs/Dashboards: Trial Orchestrator generates the executive trial dashboard (enrollment vs. plan per site, milestone timeline tracker, budget actual vs. forecast, SAE summary, data quality score); Enrollment Agent generates the enrollment funnel dashboard per site; Budget Agent generates the trial cost tracker (cost-per-patient trend, budget vs. actual by trial phase, projected completion cost); Data Management Agent generates the data quality dashboard (query rate per site, data completeness score, outstanding queries by age), Document Intelligence: The primary tool across the Protocol, Regulatory, Safety, and Data Management Agents – extracting structured data from clinical protocols, informed consent forms, SAE narratives, CRF (Case Report Form) completion instructions, regulatory guidance documents (FDA guidance https://www.fda.gov/regulatory-information/search-fda-guidance-documents, EMA guidelines https://www.ema.europa.eu/en/human-regulatory-overview/research-and-development/scientific-guidelines), site qualification reports, CSR (Clinical Study Report) templates, and prior submission packages; each agent receives only the document set relevant to its domain task, https://www.fda.gov/industry/fda-data-standards-council/electronic-submissions-gateway and EMA SPOR services https://spor.ema.europa.eu/sporwi/ submission tracking), Budget Agent (financial DW trial cost data, CRO invoice processing system), Trial Orchestrator (Veeva CTMS milestone tracking, Snowflake DW trial metrics write), Integration Workflow as Tool: Trial Orchestrator and Worker Agents call pre-built clinical operations sub-workflows – Protocol Agent (Veeva CTMS protocol deviation record creation and amendment initiation sub-workflow), Safety Agent (SAE regulatory notification package assembly and submission sub-workflow after Medical Monitor HITL), Regulatory Agent (eCTD submission package assembly and FDA/EMA submission portal upload sub-workflow after Regulatory Affairs Director HITL), Budget Agent (financial DW trial cost write and CPO budget alert sub-workflow), Enrollment Agent (CTMS enrollment milestone update sub-workflow), Watcher Tools: Trial Orchestrator monitors Veeva CTMS for new adverse event submissions, protocol deviation records, enrollment milestone updates, and submission status changes – triggering the appropriate Worker Agent within 4 hours of each clinical event; Safety Agent monitors the SAE reporting queue continuously for new SAE submissions to ensure 7-day and 15-day regulatory notification deadlines are never missed, Web Crawling: Regulatory Agent monitors FDA guidance document database, EMA scientific guideline publications, ICH guideline updates https://www.ich.org/page/multidisciplinary-guidelines, and relevant regulatory body websites for new submission requirements, format changes, and guidance updates applicable to the active trial’s therapeutic area and submission pathway; Safety Agent monitors FDA Drug Safety Communications and EMA safety referrals for new safety information relevant to the trial’s investigational product class |
Table of Contents
| Messaging: |
All 8 agents communicate via structured clinical trial event messages – the Safety Agent publishes a structured SAE event (patient ID pseudonym; event term; onset date; causality assessment; expectedness classification; regulatory notification deadline computed) to the Trial Orchestrator and Medical Monitor for HITL review; the Enrollment Agent publishes a structured enrollment status event (site ID; enrollment rate; days behind/ahead of plan; projected milestone date) to the Orchestrator for critical path impact assessment and VP Clinical Operations awareness. |
|---|---|
| Reflection: |
The Trial Orchestrator applies a reflection cycle when cross-agent findings create compound trial risk – for example; when the Data Management Agent identifies a systematic data quality issue at a site simultaneously with the Enrollment Agent flagging that site as a top-enrolling site; the Orchestrator evaluates the compound risk (high enrollment + low data quality = high pivotal trial integrity risk) and re-queries the Knowledge Base for site remediation precedents before routing the compound risk to the VP Clinical Operations with a structured risk narrative. The Safety Agent applies a mandatory reflection cycle before computing the regulatory notification deadline – re-querying the ICH E2A classification standards and verifying the expectedness determination against the current Investigator’s Brochure before confirming the notification timeline. |
| Knowledge: |
All 8 agents share a persistent clinical trial vector knowledge base containing: approved protocol language and amendment templates per therapeutic area and phase; ICH E2A/E2B adverse event classification standards and expectedness determination methodology; ICH E6 GCP compliance requirements and acceptable deviation response procedures; FDA/EMA/ICH regulatory submission requirements per submission type and eCTD module structure; site performance history from prior trials (enrollment velocity; deviation rate; data quality score per site and investigator); inclusion/exclusion criteria matching logic per protocol version; trial budget benchmarks per indication and phase (Phase I/II/III cost-per-patient benchmarks); and prior trial CSR (Clinical Study Report) and submission narratives. Indexed by trial ID; site; protocol version; indication; and regulatory pathway. |
| Execution: |
The Protocol Agent monitors Veeva CTMS for protocol deviations and tracks amendment status via API Tool Call. The Site Selection Agent scores site candidates using historical performance data from the Knowledge Base and presents a ranked shortlist via Data Analytics. The Enrollment Agent matches EHR patient records against inclusion/exclusion criteria via FHIR API and monitors enrollment funnel metrics. The Data Management Agent queries Medidata Rave EDC for data quality issues via API Tool Call and generates queries within SLA. The Safety Agent processes each SAE via Document Intelligence and routes completed narratives to the Medical Monitor for HITL review. The Regulatory Agent assembles eCTD submission packages via Document Intelligence and Integration Workflow as Tool. The Budget Agent monitors trial costs vs. budget via financial DW API Tool Call. The Trial Orchestrator delivers the weekly executive trial dashboard via Data Analytics. |
| Business Impact: |
Tufts Center for the Study of Drug Development: the average cost to develop and gain approval for a new drug is $2.6B; clinical trial operations failures (enrollment delays; data quality issues; protocol amendments; regulatory submission deficiencies) account for 35 to 40% of total drug development cost and timeline overruns. Phase III clinical trial enrollment delays average 30% longer than planned (Tufts CSDD); adding $37,000 per day in direct and indirect trial costs. The Goldfinch AI clinical operations system compresses clinical trial timelines by 20 to 30% through automated enrollment matching; proactive data quality monitoring; and real-time milestone risk identification – converting the historically reactive; siloed clinical operations function into a continuously coordinated; intelligence-driven operation. |
| Planning: |
Regulatory Agent active at IND, protocol amendment, and NDA/BLA/MAA submission milestones; Budget Agent active throughout). Schema-driven rules govern trial lifecycle stage dependencies (IND clearance before site activation, database lock before NDA package assembly) and regulatory notification deadlines (SAE: 7-day for fatal/life-threatening, 15-day for other unexpected SAEs); LLM reasoning governs protocol deviation pattern analysis, site performance narrative, safety causality assessment context, and regulatory submission narrative generation., The Trial Orchestrator uses clinical trial lifecycle stage decomposition – when a new trial is activated, the Orchestrator ingests the protocol synopsis and trial parameters and decomposes the trial lifecycle into phase-specific sub-tasks per Worker Agent (Protocol Agent active throughout; Site Selection Agent active during feasibility and startup; Enrollment Agent active during screening and enrollment; Data Management and Safety Agents active throughout data collection; |
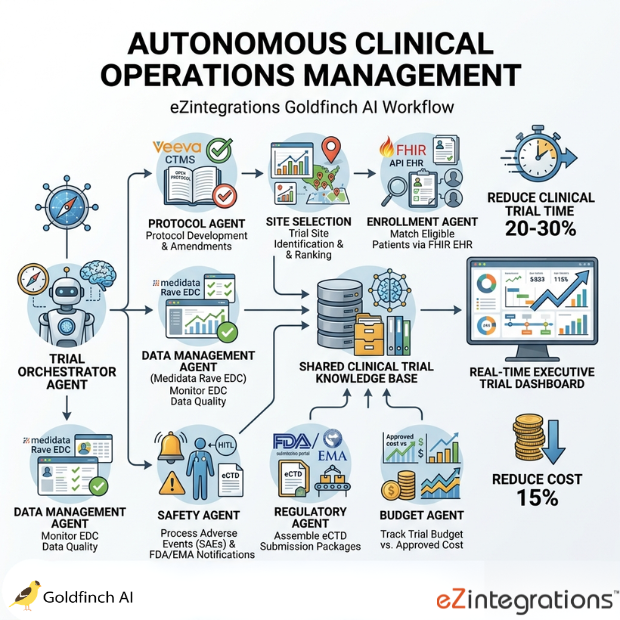
The Goldfinch AI clinical operations system from eZintegrations deploys 8 coordinated AI agents – a Trial Orchestrator plus 7 specialized Worker Agents – to manage protocol development and amendments in Veeva CTMS, identify and rank optimal trial sites, match eligible patients via FHIR EHR APIs, monitor EDC data quality in Medidata Rave, process adverse events and SAE regulatory notifications, assemble eCTD submission packages for FDA and EMA, track trial budget vs. approved cost, and deliver a real-time executive trial dashboard – reducing clinical trial time by 20 to 30% and cost by 15% per trial. eZintegrations is an enterprise automation platform covering iPaaS, AI Workflows, AI Agents, and Goldfinch AI agentic automation.
What Is Goldfinch AI Clinical Operations Automation?
Goldfinch AI clinical operations automation is a hierarchical multi-agent system where a Trial Orchestrator maintains the master trial timeline and milestone risk register across 7 domain-specific Worker Agents simultaneously – managing protocol, site, enrollment, data, safety, regulatory, and budget domains in coordination through a shared clinical trial Knowledge Base. Unlike CTMS or EDC platforms that present clinical data for operations teams to act on manually, the Goldfinch AI clinical operations system autonomously advances the trial lifecycle within configured scope, surfaces compound clinical risks across domains, and escalates every safety, protocol, and regulatory decision to the appropriate qualified professional for mandatory human review.
How Does Goldfinch AI Clinical Operations Use 8 Agents Across Veeva CTMS, Medidata EDC, FHIR, and FDA/EMA Submission Portals to Reduce Clinical Trial Time 20 to 30% and Cost by 15%?
The Protocol Agent manages deviations and amendments in Veeva CTMS. The Site Selection Agent scores sites from performance history via Data Analysis. The Enrollment Agent matches EHR patients via FHIR API. The Data Management Agent monitors EDC quality in Medidata Rave. The Safety Agent processes SAEs via Document Intelligence with mandatory Medical Monitor HITL. The Regulatory Agent assembles eCTD packages via Document Intelligence and Integration Workflow as Tool. The Budget Agent tracks trial cost vs. budget from the financial DW. The Trial Orchestrator coordinates all 8 agents through the shared clinical trial Knowledge Base.
Goldfinch AI ships with 9 native out-of-the-box agent tools. Users can add custom tools self-service beyond the 9 native tools. Tufts CSDD: average drug development cost $2.6B; trial operations failures account for 35 to 40% of overruns. This Goldfinch AI clinical operations system addresses those failure modes simultaneously.
Watch Demo
| Video Title: |
Goldfinch AI Clinical Operations | 8 Agents; Protocol to NDA Submission Across Veeva CTMS; Medidata EDC; and FHIR |
|---|---|
| Duration: |
8 to 12 minutes |
Outcome & Benefits
| Autonomy: |
75%+ of clinical trial operational tasks executed autonomously within configured scope (enrollment matching; data quality monitoring and query generation; SAE deadline computation; budget variance tracking; site performance scoring; submission package document assembly); all SAE regulatory notifications; protocol amendments; and regulatory submissions require qualified physician or Regulatory Affairs Director HITL sign-off before execution; patient eligibility assessment always includes CRA review for borderline criteria matches |
|---|---|
| Time Saved: |
Enrollment cycle time from protocol activation to first patient in from average 16 months (Tufts CSDD benchmark) reduced by estimated 20 to 30%; SAE regulatory notification from manual compilation (average 8 to 12 hours for a 15-day report) to automated narrative assembly with Medical Monitor review in under 3 hours; data management query generation from weekly manual EDC review to continuous automated monitoring with same-day query generation; submission package assembly from 4 to 8 weeks manual document collection to automated assembly in 3 to 7 business days |
| Cost Reduction: |
15% overall trial cost reduction from enrollment acceleration (Tufts CSDD: $37,000 per day of Phase III delay); data quality improvement (reduced protocol amendments from better deviation detection); and submission deficiency avoidance (average FDA Complete Response Letter costs $100M to $500M in delayed approval revenue); budget tracking automation eliminates estimated 2 to 3 FTE of trial finance management overhead per trial |
| Reliability: |
100% of SAE submissions processed with regulatory notification deadline computation; zero SAE regulatory notification deadline missed through continuous Watcher Tools monitoring; 100% of Medidata Rave EDC data quality issues detected with structured query generation; clinical trial budget variance tracked continuously vs. monthly manual reporting in prior processes |
Performance Metrics
| KPI | Before (Manual Clinical Ops) | After (Goldfinch AI Clinical Operations) | Impact |
|---|---|---|---|
| First Patient In (FPI) Timeline | 16 months average (Tufts CSDD) | 20 to 30% reduction | 3.2 to 4.8 months faster |
| SAE Notification Preparation | 8 to 12 hours manual | Under 3 hours with HITL | 75%+ faster |
| Data Query Generation | Weekly manual EDC review | Continuous automated monitoring | Same-day query generation |
| Submission Package Assembly | 4 to 8 weeks manual | 3 to 7 business days | 60 to 85% faster |
| Trial Cost vs. Budget Visibility | Monthly manual reporting | Continuous real-time tracking | Proactive variance detection |
| Enrollment Rate Visibility | Weekly site reports | Real-time per-site funnel tracking | Earlier intervention |
Technical Details
| Evaluation Metrics: |
First Patient In (FPI) timeline vs. plan (days from protocol activation to first patient enrolled); enrollment completion date vs. plan (days ahead/behind per site and overall); SAE regulatory notification on-time rate (% of SAE notifications submitted within ICH E2A deadline; 7-day and 15-day); EDC data query response rate (% of queries resolved within SLA per site); protocol deviation rate per site per visit; submission package deficiency rate (% of submissions receiving FDA/EMA requests for additional information); trial cost-per-patient vs. benchmark; budget variance at each trial milestone; Trial Orchestrator compound risk events identified and escalated vs. HITL escalation acceptance rate. |
|---|---|
| Planner Type: |
and HITL gate triggers per event type; LLM reasoning governs protocol deviation pattern analysis, site selection narrative justification, safety causality assessment narrative for Medical Monitor review context, regulatory submission narrative generation, and compound clinical risk assessment when multiple domain agents flag the same site or trial parameter simultaneously, Clinical trial lifecycle stage decomposition with LLM-hybrid execution – the Trial Orchestrator uses schema-driven rules for trial lifecycle stage dependencies (IND clearance before site activation; database lock before NDA package assembly; SAE 7-day and 15-day notification deadline enforcement from ICH E2A classification), regulatory notification timeline rules (mandatory per ICH E2A/E2B), |
| Agent Roles: |
Budget Agent: API Tool Call (financial DW trial cost data, CRO invoice system, investigator fee tracking), Data Analysis (cost-per-patient computation, cost-per-milestone, budget variance trend analysis, projected trial cost overrun at current burn rate), Data Analytics with Charts/Graphs/Dashboards (trial cost tracker: cost-per-patient trend, budget vs. actual by trial phase, projected completion cost), Knowledge Base Vector Search (trial budget benchmarks per indication and phase, CRO cost benchmarks), Enrollment Agent: API Tool Call (FHIR API https://www.hl7.org/fhir/ for EHR patient record matching at configured sites, Veeva CTMS enrollment milestone tracking), Data Analysis (inclusion/exclusion criteria matching scoring with confidence assessment, enrollment velocity and completion date projection), Data Analytics with Charts/Graphs/Dashboards (enrollment funnel dashboard per site), Knowledge Base Vector Search (inclusion/exclusion criteria matching logic per protocol version, enrollment benchmark by indication), Integration Workflow as Tool (CTMS enrollment milestone update sub-workflow), Regulatory Agent: API Tool Call (FDA Electronic Submissions Gateway https://www.fda.gov/industry/fda-data-standards-council/electronic-submissions-gateway, EMA SPOR submission services https://spor.ema.europa.eu/sporwi/, Veeva CTMS document library), Document Intelligence (prior submission packages, regulatory guidance documents, eCTD technical specifications, CSR templates, FDA Complete Response Letters for precedent analysis), Data Analysis (submission package completeness scoring per eCTD module, regulatory gap identification), Knowledge Base Vector Search (FDA/EMA regulatory submission requirements per submission type, eCTD module mapping, approved submission narratives), Integration Workflow as Tool (eCTD submission package assembly and submission portal upload sub-workflow after Regulatory Affairs Director HITL), Safety Agent: API Tool Call (Veeva CTMS SAE module, FDA MedWatch portal API https://www.fda.gov/safety/medwatch-fda-safety-information-and-adverse-event-reporting-program, EMA EudraVigilance https://www.ema.europa.eu/en/human-regulatory-overview/research-and-development/pharmacovigilance/eudravigilance), Document Intelligence (SAE narratives, Investigator’s Brochure for expectedness determination, prior safety reports), Data Analysis (SAE causality and severity scoring using ICH E2A/E2B standards, regulatory notification deadline computation), Knowledge Base Vector Search (ICH E2A/E2B AE classification standards, expectedness determination criteria, prior safety reports for the investigational product class), Integration Workflow as Tool (SAE regulatory notification package assembly and submission portal upload sub-workflow after Medical Monitor HITL), Site Selection Agent: API Tool Call (Veeva CTMS site performance data and site qualification records), Data Analysis (site scoring: enrollment velocity, deviation rate, data quality score, investigator experience, patient population access, site infrastructure), Data Analytics with Charts/Graphs/Dashboards (ranked site shortlist dashboard with scoring rationale), Knowledge Base Vector Search (site performance history from prior trials, enrollment benchmark by indication and geography), Trial Orchestrator (Coordinator): trial lifecycle stage management, milestone risk register maintenance, cross-domain compound risk assessment, VP Clinical Operations/CMO escalation routing, executive trial dashboard assembly Protocol Agent: API Tool Call (Veeva CTMS https://www.veeva.com/products/vault-ctms/ protocol version tracking and deviation records, IRB/Ethics Committee submission portal), Document Intelligence (protocol documents, informed consent forms, CRF completion instructions, amendment documentation), Data Analysis (protocol deviation pattern classification and amendment trigger scoring), Knowledge Base Vector Search (approved protocol language and amendment templates, GCP deviation response procedures) |
| Scheduling: |
Protocol Agent monitors Veeva CTMS for new deviation records at 24-hour intervals; Regulatory Agent activates at configured submission milestones (IND submission, protocol amendment submission, NDA/BLA package assembly); Budget Agent runs weekly cost variance computation and immediately on any invoice exceeding configured approval threshold; Site Selection Agent activates during feasibility phase and on-demand for site expansion decisions; Trial Orchestrator delivers weekly executive trial dashboard and immediate escalation for any milestone delay above the critical path threshold., Trial Orchestrator monitors Veeva CTMS, Medidata Rave EDC, and FHIR patient matching queue via Watcher Tools continuously – Safety Agent SAE queue monitored for regulatory notification deadline risk at 4-hour intervals (immediate trigger on new SAE submission to ensure 7-day and 15-day deadlines are never missed); Enrollment Agent runs daily enrollment velocity computation and weekly site comparison analysis; Data Management Agent monitors Medidata Rave EDC for new data entry and outstanding queries at 24-hour intervals; |
| Tool Router: |
Each Worker Agent selects its tools based on domain task: API Tool Call for CTMS/EDC/FHIR/LIMS/regulatory portal reads and writes; Document Intelligence for protocol, SAE narrative, regulatory guidance, and prior submission document analysis; Data Analysis for scoring, projection, and validation; Knowledge Base for clinical standards, site history, and regulatory requirements; Web Crawling for regulatory guidance monitoring; Data Analytics for trial dashboards; Watcher Tools for continuous clinical event monitoring; Integration Workflow as Tool for CTMS, EDC, and regulatory submission portal sub-workflows., The Trial Orchestrator routes each clinical trial event to the appropriate Worker Agent based on event type and trial lifecycle stage – new SAE submission triggers Safety Agent immediately; new protocol deviation record in CTMS triggers Protocol Agent; enrollment milestone fall-behind triggers Enrollment Agent alert and site-specific intervention assessment; new EDC data query backlog above SLA triggers Data Management Agent escalation; upcoming submission milestone triggers Regulatory Agent package assembly initiation; budget variance above threshold triggers Budget Agent alert and VP Clinical Operations notification. |
| Auditability: |
Every agent action is logged with: agent name, trial ID, patient pseudonym (where applicable), site ID, clinical event type (AE, deviation, query, enrollment, submission), tool invoked, data retrieved, recommendation generated, regulatory standard applied (ICH E2A, ICH E6 GCP, 21 CFR Part 11), confidence score, HITL status (autonomous monitoring or Medical Monitor/CRA/Regulatory Affairs Director-reviewed and signed), regulatory submission reference (FDA submission tracking number, EMA EUDRACT number), and timestamp., The Trial Orchestrator maintains a per-trial audit trail from protocol activation through submission that is fully compliant with FDA 21 CFR Part 11 (electronic records and signatures) and ICH E6 GCP (audit trail requirements for clinical investigation records). The complete audit trail is accessible via the Goldfinch AI audit dashboard with export to the eTMF for regulatory inspection readiness. All SAE processing and regulatory notification records are stored with the Medical Monitor’s review identity and sign-off timestamp for pharmacovigilance audit. The Regulatory Agent’s submission package assembly log provides the complete document provenance trail for each eCTD module for FDA/EMA pre-approval inspection. |
Connectivity and Deployment
| Supported Protocols: |
REST API (Veeva CTMS REST API; Medidata Rave EDC REST API; LIMS REST API; financial DW; FDA Electronic Submissions Gateway; EMA SPOR and EudraVigilance APIs; Snowflake DW JDBC); HL7 FHIR R4 API (EHR patient record matching at configured clinical sites – FHIR R4 compliant with SMART on FHIR authorization for site-level EHR access); Web Crawling (FDA guidance document database; EMA scientific guidelines; ICH guideline registry; FDA Drug Safety Communications); SMTP (Safety Committee SAE alert notifications; VP Clinical Operations milestone risk alerts; site enrollment performance notifications; Budget Agent variance alerts); HTTPS; OAuth 2.0; SMART on FHIR (site EHR authorization); IPSec Tunnel (on-premises CTMS; EDC; LIMS; eTMF) |
|---|---|
| Tenancy Model: |
Single-tenant per trial program is mandatory for all clinical operations deployments. Clinical trial data – patient pseudonyms; safety data; protocol documents; site performance data; and regulatory submission content – is subject to FDA 21 CFR Part 11; ICH E6 GCP; HIPAA; and GDPR (for EU subject data); all of which require strict data isolation; controlled access; and audit trail integrity. Single-tenant provides dedicated infrastructure with configurable data residency per regulatory jurisdiction (US: FDA 21 CFR Part 11; EU: GDPR Article 9 clinical trial data; ICH E6 GCP international). Multi-tenant is not available for clinical trial deployments. |
| On-Premise Supported: |
Yes – eZintegrations connects to on-premises systems (on-premises Veeva CTMS; on-premises Medidata EDC; on-premises LIMS; on-premises eTMF systems) via IPSec Tunnel. eZintegrations is a browser-based; cloud-hosted platform and does not require any on-premises software installation. |
| Security & Compliance: |
FDA 21 CFR Part 11-compliant (electronic records, electronic signatures – every HITL decision is captured with reviewer identity, timestamp, and decision rationale in an immutable audit trail; all agent actions are logged with the equivalent electronic record documentation required for a complete audit trail under 21 CFR Part 11); ICH E6(R2) GCP-compliant (audit trail requirements for all clinical investigation records – Trial Orchestrator maintains the complete per-trial agent action chronology for regulatory inspection); HIPAA-compliant (all patient data processed by the Enrollment Agent is pseudonymized at the point of FHIR API retrieval – no direct patient identifiers are stored in the Goldfinch AI system;, pseudonymization mapping maintained in the sponsor’s controlled environment); GDPR Article 9-compliant for EU clinical trial subject data (processing under explicit consent framework per EU Clinical Trials Regulation 536/2014); SOC Type II certified. RBAC enforced: CMO has full trial portfolio view; VP Clinical Operations accesses all active trial dashboards; Medical Monitor accesses Safety Agent SAE queue and HITL reviews only; Regulatory Affairs Director accesses Regulatory Agent submission packages; site CRAs access site-level enrollment and data management data only; patient data accessible only to authorized site personnel within FHIR authorization scope. |
AI Credits
| Retry / Reflection Credit Cost: |
Each Trial Orchestrator compound risk reflection cycle: ~6 to 10 additional credits per retry. Safety Agent ICH E2A classification reflection: ~5 to 8 additional credits per event. At 15% complex event rate (events requiring additional reflection due to borderline classification); add approximately 15 to 20% to the annual credit estimate. |
|---|---|
| Monthly Credit Estimate (at Typical Volume): |
Single Phase II trial (10 to 20 sites; moderate SAE volume; monthly enrollment monitoring): ~600 to 1,500 credits per month Single Phase III trial (50 to 100 sites; high enrollment and SAE volume; quarterly submissions): ~2,000 to 5,000 credits per month Portfolio of 5 active trials across phases (typical mid-size biotech): ~8,000 to 20,000 credits per month |
| Pricing Model: |
Static Platform Fee + AI Credits. Platform fee covers unlimited non-LLM orchestration across all agents (Veeva CTMS connection; Medidata EDC connection; FHIR API integration management; LIMS connection; SMTP notification dispatch; Snowflake DW writes; audit log writes). AI Credits consumed only by Goldfinch AI tool invocations and LLM reasoning cycles. |
| Credit Optimization Notes: |
Configure Data Management Agent EDC monitoring at 24-hour intervals (not real-time) – EDC data query generation does not require real-time processing and 24-hour batching reduces API Tool Call credits by 60 to 70%. Cache Knowledge Base ICH E2A classification standards and regulatory submission requirements per trial and therapeutic area for the trial duration (regulatory standards do not change within a trial cycle). For Safety Agent Document Intelligence; apply full analysis only to SAE narratives (high priority); apply Document Intelligence to AE reports only when severity or causality requires Medical Monitor attention. Configure Regulatory Agent to activate only at confirmed submission milestones; not on speculative pre-assembly checks. Batch FHIR API patient matching queries for the Enrollment Agent’s daily eligibility screening across all configured sites in a single API Tool Call per site rather than per-patient sequential queries. |
| AI Credits Required: |
Yes – Document Intelligence is the primary credit consumer per trial due to the document-intensive nature of clinical trial operations (protocols, SAE narratives, regulatory guidance documents, prior submission packages). Credit consumption scales with trial complexity, phase, and document volume. |
| LLM Steps Count: |
16 to 30 LLM-invoking steps per active trial week (Trial Orchestrator milestone risk assessment: 2 to 4 steps; Safety Agent SAE processing per event: 3 to 6 steps; Regulatory Agent submission package assembly: 4 to 8 steps; Data Management Agent EDC quality assessment: 2 to 4 steps; Enrollment Agent patient matching: 2 to 4 steps; Budget Agent variance analysis: 1 to 2 steps; reflection/retry: 1 to 3 steps per retry) |
| Per-Agent Credit Breakdown: |
Data Management Agent: 2 to 4 credits per daily EDC monitoring cycle (Medidata Rave API + data quality Data Analysis); Safety Agent: 8 to 15 credits per SAE event (Veeva CTMS SAE API + Document Intelligence SAE narrative and Investigator’s Brochure analysis + ICH E2A classification Data Analysis + notification deadline computation + Integration Workflow submission package); Regulatory Agent: 20 to 50 credits per submission package (Document Intelligence multiple regulatory documents + eCTD completeness Data Analysis + Integration Workflow assembly – highest per-event credit consumer; scales with submission complexity and document volume); Budget Agent: 3 to 6 credits per weekly cost variance computation (financial DW API Tool Call + cost-per-patient Data Analysis + variance Data Analytics), Trial Orchestrator: 4 to 8 credits per weekly cycle (milestone risk assessment + cross-agent compound risk evaluation + executive dashboard assembly); Protocol Agent: 6 to 12 credits per deviation/amendment event (CTMS API Tool Call + Document Intelligence protocol analysis + deviation pattern Data Analysis + Knowledge Base amendment template retrieval); Site Selection Agent: 10 to 20 credits per site selection engagement (CTMS site performance data API + weighted scoring Data Analysis + Data Analytics ranked shortlist dashboard); Enrollment Agent: 3 to 6 credits per weekly enrollment cycle (FHIR API patient matching + eligibility Data Analysis + enrollment funnel Data Analytics per site) |
| Goldfinch AI Tool(s) Consuming Credits: |
Document Intelligence (Protocol Agent protocol and amendment documents; Safety Agent SAE narratives, Investigator’s Brochure, prior safety reports; Regulatory Agent prior submissions, guidance documents, CSR templates – primary credit consumer; scales with document volume), API Tool Call (all 7 Worker Agents per CTMS/EDC/FHIR/LIMS/regulatory portal/financial DW call), Data Analysis (Site Selection scoring; Enrollment eligibility matching and velocity projection; Data Management EDC quality; Safety ICH E2A classification; Budget cost variance;, Orchestrator milestone risk – per computation cycle), Knowledge Base Vector Search (all 8 agents per clinical standards and trial context query), Web Crawling (Regulatory Agent FDA/EMA/ICH guidance monitoring; Safety Agent FDA Drug Safety Communications – per crawl cycle), Watcher Tools (Trial Orchestrator continuous CTMS, EDC, and SAE queue monitoring), Data Analytics with Charts/Graphs/Dashboards (Site Selection ranked shortlist; Enrollment funnel per site; Budget cost tracker; Orchestrator executive trial dashboard – per render), Integration Workflow as Tool (Protocol CTMS deviation record; Safety SAE notification submission; Regulatory eCTD package assembly and upload; Enrollment CTMS milestone update; Budget financial DW write – per sub-workflow) |
| Credit Consumption Model: |
Event-driven per clinical trial event (each new SAE, protocol deviation, enrollment milestone, EDC query batch, budget variance event triggers an agent cycle); weekly continuous monitoring for Enrollment, Data Management, and Budget Agents; milestone-triggered for Regulatory Agent (activated at IND, protocol amendment, NDA/BLA milestones); annual for Site Selection Agent (feasibility phase); total trial credit cost scales with trial complexity, phase, number of sites, and document volume |
FAQ
1. What is the Autonomous Clinical Operations Management system and what does it automate end to end?
The Goldfinch AI clinical operations system from eZintegrations deploys 8 coordinated AI agents — a Trial Orchestrator and 7 domain Worker Agents — to manage protocol development and amendments in Veeva CTMS (Protocol Agent), identify and rank optimal trial sites (Site Selection Agent), match eligible patients via FHIR EHR APIs (Enrollment Agent), monitor EDC data quality in Medidata Rave (Data Management Agent), process adverse events and SAE regulatory notifications with mandatory Medical Monitor HITL (Safety Agent), assemble eCTD submission packages for FDA and EMA (Regulatory Agent), and track trial cost vs. approved budget (Budget Agent) — reducing clinical trial time by 20 to 30% and cost by 15%. Tufts CSDD: average drug development cost is $2.6B; trial operations failures account for 35 to 40% of overruns.
2. How does the multi-agent architecture work?
The Trial Orchestrator maintains the master trial timeline and milestone risk register and coordinates all 7 Worker Agents through a shared clinical trial Knowledge Base containing ICH E2A/E2B classification standards, GCP requirements, FDA/EMA submission requirements, site performance history, and approved protocol language. All 8 agents run simultaneously — the Safety Agent monitors the SAE queue continuously for regulatory deadline risk while the Enrollment Agent tracks enrollment velocity per site, the Data Management Agent monitors EDC data quality, and the Budget Agent tracks cost variance. The Orchestrator cross-references domain agent signals for compound risks (high-enrolling site with low data quality) and escalates structured risk narratives to the VP Clinical Operations.
3. Which Goldfinch AI tools does this system use?
The system uses 8 of Goldfinch AI's 9 native tools: Document Intelligence (Protocol Agent protocol and amendment documents; Safety Agent SAE narratives, Investigator's Brochure, and prior safety reports; Regulatory Agent prior submissions and regulatory guidance — primary credit consumer), Knowledge Base Vector Search (all 8 agents — ICH E2A standards, GCP requirements, FDA/EMA submission requirements, site history, protocol language), API Tool Call (all 7 Worker Agents — Veeva CTMS, Medidata Rave EDC, FHIR API, LIMS, FDA/EMA portals, financial DW), Data Analysis (site scoring; eligibility matching; EDC quality; ICH E2A classification; cost variance; milestone risk), Watcher Tools (Trial Orchestrator continuous SAE queue and trial event monitoring), Web Crawling (Regulatory Agent FDA/EMA/ICH guidance; Safety Agent FDA Drug Safety Communications), Data Analytics (site selection dashboard; enrollment funnel; budget cost tracker; executive trial dashboard), and Integration Workflow as Tool (SAE notification submission; eCTD package assembly; CTMS enrollment milestone; financial DW write). Users can add eTMF, RTSM/IWRS, PRO platforms, and RWE database APIs self-service.
4. How does the system ensure data accuracy and handle errors?
The Trial Orchestrator applies a reflection cycle when cross-agent signals create compound trial risk — if the confidence score falls below 0.75 on any milestone risk assessment, it re-queries the Knowledge Base for precedents, retries up to 3 times, and escalates to the VP Clinical Operations with full context. The Safety Agent applies a mandatory reflection cycle before computing each SAE regulatory notification deadline — re-querying the ICH E2A classification standards and verifying expectedness against the current Investigator's Brochure. The Enrollment Agent routes all inclusion/exclusion matches below 0.80 confidence to a CRA for review before any patient outreach is initiated. All SAE regulatory notifications and regulatory submissions always require qualified physician or Regulatory Affairs Director sign-off before execution.
5. What types of data and documents does this system process?
The system processes: Veeva CTMS protocol versions, deviation records, site qualification data, and enrollment milestones; Medidata Rave EDC patient data and query records (pseudonymized); FHIR R4 EHR patient records (pseudonymized at retrieval, matched against inclusion/exclusion criteria); LIMS sample data; SAE narratives, Investigator's Brochures, and prior safety reports (Safety Agent Document Intelligence); clinical protocols, informed consent forms, CRF completion instructions, and protocol amendments (Protocol Agent Document Intelligence); prior regulatory submission packages, FDA/EMA guidance documents, and eCTD templates (Regulatory Agent Document Intelligence); trial financial data from the financial DW (Budget Agent).
6. Who uses this system and in which departments?
Daily operators include the Clinical Program Director (receives Trial Orchestrator weekly trial dashboard and milestone risk alerts), Medical Monitor (reviews Safety Agent SAE narratives and provides HITL causality and expectedness assessment — mandatory sign-off before regulatory notification), Clinical Research Associates (review Enrollment Agent borderline eligibility matches and Data Management Agent site-level query alerts), and Regulatory Affairs Director (reviews Regulatory Agent submission packages and provides HITL sign-off before any FDA/EMA submission). Executive stakeholders — the VP Clinical Operations and CMO — receive the weekly executive trial dashboard and immediate escalation for critical path milestone delays. The Safety Committee receives all SAE HITL review requests.
7. How does the safety layer and human oversight work?
HITL is mandatory for all regulated clinical trial decisions: every SAE requires Medical Monitor and Safety Committee review before regulatory notification (no autonomous SAE submission); every protocol amendment requires Medical Monitor and IRB/Ethics Committee approval; every regulatory submission requires Regulatory Affairs Director and CMO sign-off; every borderline enrollment eligibility match (below 0.80 confidence) requires CRA review. The Safety Agent applies a mandatory ICH E2A reflection cycle on every SAE before computing the notification deadline. After 3 Trial Orchestrator retries below 0.75 confidence, the VP Clinical Operations receives a structured risk escalation. All HITL decisions are logged with reviewer identity and timestamp for FDA 21 CFR Part 11 and ICH E6 GCP compliance.
8. What are the key business benefits and executive KPIs improved?
Key benefits include: clinical trial timeline reduction of 20 to 30% from automated enrollment matching and proactive milestone risk identification (Tufts CSDD: $37,000 per day of Phase III delay cost), 15% overall trial cost reduction, SAE regulatory notification preparation from 8 to 12 hours manual to under 3 hours with HITL, submission package assembly from 4 to 8 weeks to 3 to 7 business days, 100% SAE regulatory notification deadline compliance from continuous monitoring, EDC data quality monitoring from weekly to continuous with same-day query generation, and the VP Clinical Operations shifts from compiling status from 5 disconnected systems to reviewing a single continuously updated cross-domain trial intelligence dashboard.
Resources
| Blog: |
Pharma Integration Platform: Connect SAP Veeva LIMS & Compliance Systems |
|---|---|
| Platform Overview: |
eZintegrations Platform – Enterprise iPaaS, AI Workflows & Agentic AI |
| Demo: |
Book a Demo |
| Goldfinch AI Platform: |
Agentic AI Platform — Goldfinch AI by eZintegrations |
Case Study
| Industry: |
Biotechnology / Mid-Size Global Biotech |
|---|---|
| Problem: |
Data quality: the 62-site Phase III program had an average outstanding query rate of 28% (28% of data points across all sites had an open query pending site response); industry benchmark for well-managed pivotal trials: below 5%; Regulatory submissions: the NDA package for the lead program was estimated to require 22 weeks of manual assembly; the prior NDA submission (6 years earlier) had received an FDA Complete Response Letter citing 14 data presentation deficiencies – each deficiency had taken an average of 8 weeks to resolve., 12 of the 62 sites accounted for 68% of enrollment (the remaining 50 sites were under-enrolling relative to their feasibility commitments); the Clinical Program Director had no systematic way to identify which of the 50 under-enrolling sites had recoverable enrollment potential vs. which required replacement; Safety: the team processed an average of 18 SAEs per month across the 3 programs; average time from SAE receipt to notification package submission: 11.4 hours for 15-day reports; in the prior year, 3 SAE notifications had been submitted 1 to 2 days late – each triggering an FDA information request;, A mid-size global biotech with 3 active Phase II/III oncology programs and $780M in annual R&D spend operated its clinical operations function across a team of 48 clinical operations professionals (8 Clinical Program Directors, 18 CRAs, 12 Data Managers, 6 Regulatory Affairs staff, 4 Pharmacovigilance staff). Key clinical operations gaps identified by the COO in a program review: Enrollment: The lead Phase III program (680 patients, 62 active sites across 14 countries) was running 31% behind the enrollment plan at the 18-month mark – projected to miss the primary completion date by 14 months; |
| Solution: |
Deployed the eZintegrations Goldfinch AI clinical operations system across all 3 active programs in 31 business days. Veeva CTMS connected via REST API (protocol versions, deviation records, site qualification data, enrollment milestone tracking, SAE module) for all 3 programs. Medidata Rave EDC connected via REST API (data query API, outstanding query tracking, data completeness metrics) for the Phase III and Phase II programs. FHIR R4 API configured at 52 of 62 Phase III sites (10 sites used non-FHIR-compatible EHR systems – Enrollment Agent configured for manual site reporting at those 10 sites). LIMS connected via REST API for sample data validation. Financial DW connected via JDBC for Budget Agent trial cost tracking. Knowledge Base Vector Search loaded with: ICH E2A/E2B complete adverse event classification standards,, ICH E6(R2) GCP requirements, FDA eCTD technical specifications and module mapping for NDA oncology submissions, EMA Module 5 clinical study report requirements, site performance history for all 3 programs including prior Phase I and Phase II sites (64 sites, 3 years of performance data), inclusion/exclusion criteria matching logic for all 3 active protocols (3 protocol versions each), prior NDA CRL deficiency list (14 items), and budget benchmark costs for Phase III oncology programs (per-patient cost benchmarks by region and site type). Safety Agent configured for 7-day and 15-day regulatory notification deadline enforcement from ICH E2A classification. All SAE HITL: Medical Monitor and VP Pharmacovigilance review required before any FDA MedWatch or EudraVigilance submission. FHIR authorization: SMART on FHIR configured with site-level authorization at each connected EHR site; patient data pseudonymized at FHIR API retrieval. |
| Outcome: |
After 8 months (all 3 programs): Phase III enrollment: 31% behind plan at deployment to 8% behind plan at month 8 – projected miss reduced from 14 months to 3.5 months. Site Performance: Trial Orchestrator + Enrollment Agent identified 18 of the 50 under-enrolling sites as having structural enrollment barriers (insufficient patient population, investigator capacity constraints) vs. 32 sites with recoverable enrollment potential (inadequate patient identification processes, delayed IRB activation). 14 sites were replaced or enhanced based on the Enrollment Agent’s site scoring analysis – generating 180 additional patients enrolled in months 5 to 8. SAE processing:, average time from SAE receipt to notification package ready for Medical Monitor review from 11.4 hours to 2.6 hours. Zero late SAE notification submissions in 8-month period (vs. 3 in prior year). Data quality: outstanding query rate from 28% to 6.2% (below the industry benchmark of 5% target, approaching it within the 8-month period). NDA package assembly: Regulatory Agent assembled the Phase III NDA draft package in 9 business days (vs. 22-week estimate for manual assembly). Regulatory Affairs Director review and finalization added 3 weeks – total NDA package time 24 business days vs. prior program’s 22 weeks. |
| ROI: |
Phase III enrollment acceleration (14-month miss reduced to 3.5-month miss, recovering 10.5 months of delay): at $37,000/day Phase III cost (Tufts CSDD), 10.5 months x 30 days x $37,000 = $11.6M in recovered trial cost. SAE late notification avoidance: each FDA information request from a late submission had previously required an estimated 6 weeks of regulatory team response time at $85,000/week = $510,000 per event; 3 late submissions avoided = $1.53M. Data quality improvement (28% to 6.2% query rate):, reduced estimated database lock delay by 8 weeks at $37,000/day = $20.7M in Phase III completion schedule acceleration (partial credit: estimated $12.4M for the query-rate-attributable component of schedule compression). NDA package assembly: 22 weeks to 24 business days, freeing 18 weeks of Regulatory Affairs staff time = estimated $1.8M. CRL deficiency prevention (prior program: 14 deficiencies; Regulatory Agent prior CRL analysis used to structure current submission): estimated $8M to $20M in avoided approval delay value if one CRL deficiency is avoided. Internal clinical operations team efficiency: estimated 12 FTE-weeks per month freed from manual status compilation across 3 programs = $1.2M annually. Total 8-month conservative ROI: $31.16M. Deployment cost: $225,000. Payback period: under 1 week. |
Related products
-
How to Automate New Product Development Using Multi-Agent AI Stage-Gate Orchestration
 $150.00
Download
$150.00
Download
-
How to Automate IT Operations and Incident Response Using Multi-Agent AI Systems
 $150.00
Download
$150.00
Download
-
How to Automate 2-Way Verification Between Purchase Orders and Invoices
 $0.00
Download
$0.00
Download
-
How to Build an AI Agentic Order-to-Cash System
 $150.00
Download
$150.00
Download

{kind=link}